English
English  Polski
Polski  Čeština
Čeština  Deutsch
Deutsch  Español
Español  Français
Français  Ελληνικά
Ελληνικά  Hrvatski
Hrvatski  Italiano
Italiano  Lietuviškai
Lietuviškai  Magyar
Magyar  Nederlands
Nederlands  Português
Português  Română
Română  Slovenčina
Slovenčina  Svenska
Svenska  Türkçe
Türkçe  Русский
Русский How to Read an Eyeglass Prescription: A Complete Guide for Optical Staff
Ever handed a patient their new glasses only to realize you’ve been staring at their prescription for the third time, double-checking those numbers? You’re not alone. Even seasoned optical staff occasionally pause when faced with handwritten prescriptions, faded faxes, or unusual notations.
Reading an eyeglass prescription correctly isn’t just about avoiding mistakes—it’s about being the bridge between what the eye exam measured and what your patient actually sees through their new lenses. Think of yourself as the interpreter who turns clinical shorthand into comfortable, clear vision.
Key Insights
- Prescriptions contain 5-7 core fields: SPH, CYL, Axis, ADD, Prism, Base, and PD—each serving a specific optical purpose
- Every field has a job: Sphere corrects nearsightedness or farsightedness, cylinder handles astigmatism, ADD addresses presbyopia, and prism fixes alignment issues
- Plus and minus signs matter: A minus SPH means myopia (nearsighted), a plus means hyperopia (farsighted)—mixing these up completely reverses the correction
- Axis without cylinder is meaningless: These two values always work together; if you see CYL, you must have Axis
- Contact lens prescriptions are different: They include base curve, diameter, and brand—never interchangeable with glasses prescriptions
- PD is critical for comfort: Pupillary distance aligns the optical centers with your patient’s pupils, especially important for higher prescriptions
- Software prevents common errors: Digital prescription management enforces required fields and catches impossible combinations before ordering
What Actually Is an Eyeglass Prescription?
An eyeglass prescription is a written, signed, and dated order from an optometrist or ophthalmologist specifying exactly how much optical power each lens needs to correct a patient’s refractive error. It’s both a clinical document and a legal requirement—in both Canada and the US, you can’t dispense prescription eyewear without one.
Prescriptions typically expire after 1-2 years, depending on your jurisdiction and the prescriber’s clinical judgment. US regulations require prescribers to automatically give patients their spectacle prescription after the exam, while Canadian provincial regulations govern how opticians may dispense from them.
Think of a prescription as a recipe: the eye doctor does the measuring and diagnostic work, writes down the formula, and then optical staff like you turn those numbers into actual, wearable eyewear. Your job is to read that recipe accurately and deliver exactly what was ordered.
Decoding the Standard Prescription Layout
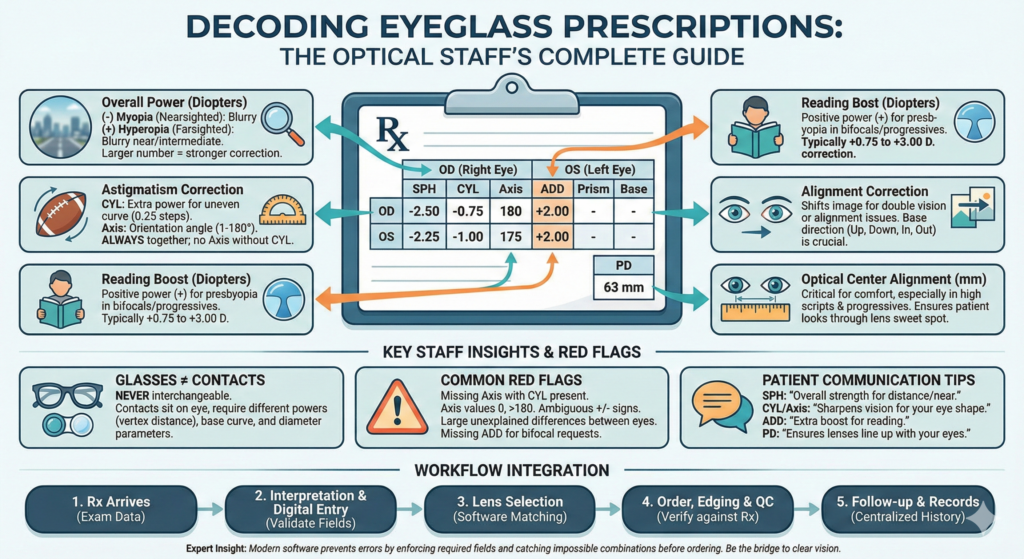
Most eye prescriptions follow a consistent table format with one row per eye and multiple columns for different parameters. Here’s what you’ll typically see:
| Field | Full Name | What This Number Means |
| OD | Oculus Dexter (right eye) | Right eye measurements—usually the top row |
| OS | Oculus Sinister (left eye) | Left eye measurements—usually the bottom row |
| SPH | Sphere | Overall lens power in diopters (+ for farsighted, − for nearsighted) |
| CYL | Cylinder | Additional power for astigmatism correction |
| Axis | Axis | Angle (1–180°) showing where cylinder power is applied |
| ADD | Addition | Extra plus power for reading in bifocals/progressives |
| Prism | Prism | Power to correct eye alignment issues |
| Base | Base Direction | Where the prism is oriented (up, down, in, out) |
| PD | Pupillary Distance | Distance between pupil centers in millimeters |
Here’s a real-world example of what a complete prescription might look like:
| Eye | SPH | CYL | Axis | ADD | Prism | Base |
| OD (right) | −2.50 | −0.75 | 180 | +2.00 | — | — |
| OS (left) | −2.25 | −1.00 | 175 | +2.00 | — | — |
| PD: 63 mm |
Modern prescription entry software mirrors this exact layout, so your staff can enter data without friction—no hunting for where to put the axis value or wondering if ADD is optional.
Breaking Down Each Field: From Numbers to Real Vision
Sphere (SPH) – The Foundation
SPH tells you the primary lens power needed, measured in diopters. This is the most important number on any prescription.
- Negative SPH (like −2.00): Patient is nearsighted—struggles to see distant objects clearly
- Positive SPH (like +2.00): Patient is farsighted—needs help with near or intermediate tasks
- Higher absolute values = stronger correction needed
The further from zero, the more powerful the lens. A prescription of −0.50 is mild; −6.00 is quite strong. When explaining to patients, you might say: “Your numbers show moderate nearsightedness, which is why things get blurry past about 10 feet without your glasses.”
Cylinder (CYL) and Axis – The Astigmatism Duo
Cylinder describes extra power needed in one meridian to correct astigmatism, which happens when the cornea or lens has uneven curvature—more like a football than a basketball.
CYL and Axis always appear together. If you see a CYL value, there must be an axis. If there’s no CYL, the patient either has no clinically significant astigmatism or it’s not being corrected.
- CYL values are usually in 0.25 diopter steps (like −0.75, −1.50, −2.25)
- Axis ranges from 1 to 180 degrees
- Axis describes orientation only, not strength
Common axis values you’ll see:
- 90° = vertical meridian
- 180° = horizontal meridian
- Anything in between = oblique astigmatism
When talking to patients: “Your eyes are slightly oval-shaped rather than perfectly round, so we’re adding a bit of extra power at this specific angle to sharpen things up.”
Addition (ADD) – Reading Power
ADD is extra magnifying power for near tasks, written as a positive number and used in bifocals, progressives, or reading glasses. Most presbyopic adults need somewhere between +0.75 and +3.00 diopters of ADD.
This number represents how much additional help your patient needs for close-up work on top of their distance prescription. Someone with +2.00 ADD needs significant near-vision support; someone with +1.00 is just starting to experience presbyopia.
Patient-friendly version: “This is how much extra boost we’re adding at the bottom of your lenses so you can read comfortably without straining.”
Prism and Base – Alignment Correction
Prism is prescribed to correct eye alignment problems or relieve double vision by shifting the image one eye sees. Most everyday prescriptions have no prism at all.
When prism is present:
- Prism amount is written as a decimal (0.5, 1.0, 2.0)
- Base direction shows how the lens is oriented: up, down, in (nasal), or out (temporal)
- Small amounts like 0.5 or 1.0 are common
This is specialized correction for binocular vision issues—think strabismus, convergence problems, or post-injury rehabilitation.
7-day free trial
Got Any Questions? Let us know in the Contact Us form below.
Pupillary Distance (PD) – The Alignment Key
PD measures the distance between your pupil centers, usually 55–70 mm for adults and smaller for children. This ensures the optical centers of the lenses match where your patient actually looks through them.
Accurate PD is essential, especially for:
- Higher prescriptions (larger errors magnify discomfort)
- Progressive lenses (narrow reading zones demand precision)
- Multifocal designs
Some prescriptions list PD separately as monocular measurements (right PD + left PD), while others give one binocular PD number. When managing client data digitally, you can store both formats and let the system calculate what the lab needs.
Expert’s Voice
“The most common mistake I see isn’t mathematical—it’s assumptions. Staff assume a missing axis was just forgotten, or that a smudged plus sign ‘probably’ means minus because the patient is young. Never guess. If something looks off, call the prescriber. Your patients’ comfort and safety depend on getting every detail exactly right, and modern software should prevent these gaps before you even reach the ordering stage.”
Adam Smith, Product Manager @ Glasson
How Numbers Are Actually Measured
Sphere, cylinder, and ADD are measured in diopters and typically written in quarter-diopter steps (0.25 D increments). So you’ll see values like −1.25, −2.50, +1.75—but rarely odd numbers like −1.37 in spectacle prescriptions.
Axis values are always whole numbers from 1 to 180. They represent angles, not power. For example:
- 180° means the cylinder is oriented horizontally
- 90° means it’s vertical
- 45° or 135° are oblique angles
Prism is measured in prism diopters, commonly with one decimal place (0.5, 1.0, 2.5). The base direction (up, down, in, out) tells you how the lens bends light.
PD is a linear distance in millimeters. Adult PDs typically fall between 55 and 70 mm, while children’s measurements are smaller.
Understanding these measurement systems helps you spot impossible values—like axis 0 or 200, or a prism value without a base direction—before they turn into ordering mistakes.
Common Notation Variants You’ll Encounter
Plus vs. Minus Cylinder Format
Here’s something that trips up newer staff: the same lens can be written two different ways.
In North America, optometrists usually write prescriptions in minus-cylinder format, while some ophthalmologists prefer plus-cylinder. The actual lens is identical—only the notation changes.
Example of the same correction written both ways:
| Format | SPH | CYL | Axis |
| Minus cylinder | −2.25 | −1.50 | 180 |
| Plus cylinder | −3.75 | +1.50 | 90 |
Both describe a lens with −2.25 D power horizontally and −3.75 D power vertically. Same optical effect, different notation.
Transposition involves three steps:
- Add sphere and cylinder to get new sphere
- Change the sign of the cylinder
- Add or subtract 90° from the axis (keeping it between 1–180)
When you’re using integrated lens selection software, the system handles transposition automatically and searches for lenses in both formats to maximize your catalog options.
DS (Diopters Sphere) Notation
Some prescribers write “D.S.” after the sphere power when there’s no astigmatism correction—like −3.00 D.S.—to confirm the cylinder wasn’t accidentally omitted. This is purely a notation choice and doesn’t change what you order.
Want to see Glasson's full potential?
Book a presentation
Red Flags: Catching Problems Before Ordering
Regulatory Completeness Checks
Before you dispense, verify these required elements:
- Patient name matches your records
- Prescriber name and credentials are clear
- Exam date is present
- Expiration date (if given) hasn’t passed
- Prescription type clearly states “spectacles” vs. “contact lens“
In Ontario, for example, spectacle prescriptions must be written, signed, and dated by a College of Optometrists member. US regulations require doctors to provide the prescription without extra fees or conditions, though expiration rules vary by state.
Optical Red Flags That Need Clarification
Watch for these warning signs:
Impossible combinations:
- Axis present but CYL is blank (or vice versa)
- Axis values of 0, 190, or anything outside 1–180
- Ambiguous plus/minus signs, especially on faded faxes
Unusual patterns:
- Wildly different values between right eye and left eye without notes (large anisometropia)
- Distance and near sections that don’t align mathematically with the stated ADD
- Prescriptions that look like contact lens orders (BC, DIA, brand listed) when the patient ordered glasses
Missing critical data:
- No PD listed for progressive lenses
- ADD missing when patient requested bifocals
- Unclear lens type designation
Because Glasson captures prescriptions through structured fields rather than free-text boxes, it can enforce rules like “axis required when CYL is entered” and prevent invalid ranges before you move to lens selection.
Why Eyeglass and Contact Lens Prescriptions Aren’t Interchangeable
Your patients check their phones about 96 times per day—and at least once a week, one of them will ask: “Can’t you just use my glasses prescription for contacts?”
The answer is always no, even when the numbers look similar.
Three critical differences:
- Vertex distance matters
Glasses sit about 12–14 mm from the cornea, while contact lenses sit directly on the eye. For higher prescriptions (typically above ±4.00 D), the effective power needs adjustment. A −5.00 D glass lens becomes roughly −4.75 D as a contact. - Fit parameters exist only for contacts
Contact lens prescriptions include base curve (BC), diameter (DIA), brand, material, and replacement schedule. These determine comfort, oxygen transmission, and whether the lens stays centered on the eye. None of these appear on glasses prescriptions. - Separate exams are required
Many clinics emphasize that patients need distinct evaluations for each modality rather than “converting” one prescription into the other. Eye health assessments, tear film evaluation, and fitting measurements are unique to contact lens exams.
When a patient asks about switching: “Your glasses prescription tells us how strong your lenses need to be. A contact lens prescription adds details about fit and lens type, so we can’t safely swap one for the other. You’ll need a separate contact lens exam.”
Modern optical practice software keeps both prescription types in the same client record, making it easy to compare them and track when each needs renewal.
Patient-Friendly Language That Actually Works
Your patients don’t need a lecture on optics—they need simple answers.
When explaining SPH:
“This number shows how strong your prescription is overall. A minus sign means you’re nearsighted—you see better up close than far away. A plus sign means you’re farsighted and need help with nearby tasks.”
When explaining CYL and Axis:
“These two numbers handle your astigmatism. Your eye is slightly more rugby-ball shaped than basketball-shaped, so we add power at a specific angle to sharpen everything up.”
When explaining ADD:
“This is the extra boost we’re adding to the bottom part of your lenses to help with reading and screen work as your eyes naturally age.”
When explaining PD:
“This is simply the distance between your pupils in millimeters, so we can line the lenses up exactly with your eyes.”
Emphasize that none of these numbers alone say whether someone has “good eyes” or “bad eyes”—they’re just data points to build lenses that match that person’s unique visual needs.
Centralized client records let you quickly pull up prior prescriptions to show patients how their numbers have shifted over time, which helps explain why they might notice bigger changes in some visits than others.
Special Cases: Kids, High Prescriptions, and Prism Wearers
Pediatric Prescriptions
Children’s prescriptions often change more frequently than adults’, with goals that include preventing amblyopia and supporting binocular development, not just providing clear vision.
Common pediatric patterns:
- Relatively low ADD values in bifocal designs for accommodative esotropia
- Prism prescribed to manage strabismus or improve binocular function
- Smaller PD measurements (often 45–55 mm)
High Prescriptions
For prescriptions above ±6.00 D, small errors multiply. You need:
- Precise PD measurements (even 1 mm off causes noticeable discomfort)
- High-index lens materials to reduce thickness
- Careful frame selection to minimize edge thickness
- Extra attention to vertex distance when converting to contacts
Prism Wearers
Patients with prism correction often have complex visual histories—post-injury, neurological conditions, or longstanding strabismus. When you see prism on a prescription:
- Verify the prism amount AND base direction before ordering
- Document whether it’s horizontal (prism base in/out) or vertical (base up/down)
- Check if it’s temporary (rehabilitation) or permanent
- Note any special lens positioning requirements
For all these cases, remember: opticians interpret and fill prescriptions but don’t diagnose or change them. When something looks inconsistent, coordinate with the prescribing eye doctor.
Test Glasson for 7 days free of charge
Any questions? Leave your contact details and we'll call you back.
Where Prescription Reading Fits in Your Daily Workflow
Reading a prescription correctly is just the front door of a smooth optical workflow. Here’s how it connects to everything else you do:
Step 1: Prescription Arrives
The optometrist completes the eye exam, records refraction data, and releases the signed prescription to the patient or transmits it to your optical store.
Step 2: Interpretation and Entry
Your optical staff reads the prescription, identifies whether it’s for distance, near, or multifocal use, and confirms any special instructions like “progressives only” or “SV near for computer work.”
Digital prescription entry mirrors the paper format you’re already familiar with—SPH, CYL, Axis, ADD, PD—reducing the chance of mis-keying data.
Step 3: Lens Selection
This is where software makes the biggest difference. Glasson’s lens search engine analyzes over three million lens combinations, matching your entered prescription with catalog data to surface suitable options in under a second.
The system handles over 22,000 combinations of visual defects, helping you compare indices, materials, and coatings without flipping through paper catalogs.
Step 4: Order, Edging, and Quality Check
Once you’ve chosen a lens design, complete the sale and order directly from within the system—no re-entering data into multiple platforms.
When glasses return from the lab, verify that measured powers, axes, prism, and PD match the prescription, then physically fit the eyewear to the patient.
Step 5: Follow-Up and Records
Integrated practice management stores exam results, prescriptions, and purchase history in one centralized record, making it easy to check old prescriptions, manage recalls, and support future lens upgrades.
FAQ

1. What does a negative number on my eyeglass prescription mean?
A negative sphere (SPH) value indicates nearsightedness (myopia)—you see nearby objects clearly but distant things appear blurry. The higher the negative number, the stronger the correction needed for distance vision.
2. Can I use my eyeglass prescription to order contact lenses?
No. Contact lens prescriptions include additional parameters like base curve, diameter, and brand that aren’t on glasses prescriptions. You need a separate contact lens exam and prescription.
3. What if my prescription doesn’t list PD?
Pupillary distance is critical for proper lens alignment. If it’s not on your prescription, ask your optical staff to measure it before ordering. Most practices measure PD as part of the dispensing process.
4. How often should I update my eyeglass prescription?
Most prescriptions expire after 1–2 years, but you should get an eye exam whenever you notice vision changes. Children and seniors may need more frequent updates.
5. What does “axis” mean on my prescription?
Axis (measured 1–180 degrees) indicates the angle where astigmatism correction is applied. It only appears when there’s a cylinder (CYL) value and describes orientation, not power strength.
6. Why are the numbers different for my left and right eyes?
It’s completely normal for your right eye and left eye to need different corrections. Each eye has unique characteristics, and prescriptions are tailored individually for optimal vision.
7. What does ADD mean on my prescription?
ADD (addition) is extra magnifying power for near vision tasks like reading, used in bifocals, progressives, or reading glasses. It’s always a positive number, typically between +0.75 and +3.00 diopters.
8. Can I read your eye prescription without an optometrist?
You can read the numbers and abbreviations on your prescription, but only a licensed eye care professional can interpret what those values mean for your eye health and determine the appropriate correction.
9. What happens if my prescription is entered wrong?
Incorrect prescription entry can cause headaches, eye strain, blurred vision, or discomfort. This is why optical staff verify all data and why digital entry systems include validation checks before ordering.
10. Do I need prism if I have double vision?
Prism correction can help manage double vision caused by eye alignment issues, but only your eye doctor can determine if it’s appropriate. Not all cases of diplopia require prism lenses.